




ICU Management & Practice, Volume 23 - Issue 3, 2023
 PRINT OPTIMISED
PRINT OPTIMISED
Together we must reduce the impact of the healthcare sector and shift towards a circular economy. This paper describes the shift of three ICU environmental hotspots: gloves, gowns, and CRRT bags.
Introduction
The healthcare sector is one of the most carbon-intensive sectors, contributing to 4.4% of global net greenhouse gas emissions and toxic air pollutants (Karliner et al. 2022). Around 71% of emissions are primarily derived from the production, transport, and disposal of medical products such as pharmaceuticals, medical devices, personal protective equipment (PPE), hospital equipment, and instruments. The Netherlands is above the global average, with 7% of its national footprint associated with the healthcare sector (Gupta Strategists 2022). Hospital care results per year in 3.8 kilotons of extracted materials, 17.6 kilotons of CO2 emissions and 4803 kilotons of waste (Steenmeijer et al. 2022). Zooming in on the waste, this consists of 15% hazardous materials (e.g. blood and infected materials) and 85% general hospital waste, of which 55% is plastics (WHO 2018). In the last decade, there was a tendency to increase efficiency and prevention of iatrogenic infection. Therefore, there was a shift to single-use products, especially in the operating room and the intensive unit (ICU). In these departments, most of the (plastic) waste is generated (Hunfeld et al. 2022).
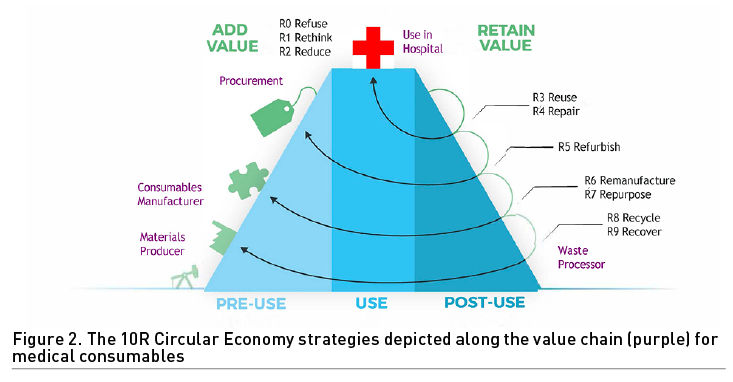
Given the current climate crisis, we must start working towards more holistic approaches to reduce the impact of the healthcare sector and shift towards a circular economy (Hinrichs-Krapels et al. 2022). We discuss three relevant approaches. First, a circular economy contains three core principles: (1) design out waste and pollution, (2) keep products and materials in use for as long as possible, and (3) regenerate natural systems (Ellen MacArthur Foundation 2020). While simple in theory, there are many complexities and trade-offs when shifting towards circular practices. Second, the 7 Pillars of the Circular Economy framework (materials, energy, water, biodiversity, human society and culture, health and well-being, and generating value) can be used as a holistic lens to map or to describe sustainability issues and to identify environmental hotspots (Kirchherr et al. 2017). Third, based on these environmental issues and hotspots, the 10R strategies can be used as a starting point for circular interventions by healthcare staff (Reike et al. 2018). The 10Rs represent Refuse, Rethink, Reduce, Reuse, Repair, Refurbish, Remanufacture, Repurpose, Recycle and Recover. Refuse (meaning not buying/using the product in the first place) is the strategy with the highest impact in the hierarchy of circular interventions, while Recover (generating energy from incineration of waste) represents the strategy with the lowest impact.
In the transition from a linear to a circular system, knowledge about the environmental impact of products and actions is needed in order to determine environmental hotspots and to use the 10R strategies. This knowledge can be obtained through so-called Life Cycle Assessments (LCA) or a Material Flow Analysis (MFA). LCAs involve the analysis of the environmental impact of natural resource extraction, manufacturing, packaging, transport, use/reuse, and recycling/waste disposal of certain products or processes (McGain et al. 2020). LCAs related to intensive care medicine have been performed for reusable central venous catheter insertion kits and septic ICU patients in the United States and Australia (McGain et al. 2020; McGain et al. 2018). An LCA of all the activities occurring within the entire ICU would be a considerable undertaking, though not impossible. Another method is the Material Flow Analysis (MFA). An MFA provides a quantitative understanding of all the goods and waste flows that enter and leave the system. It can be used to manage resources and waste flows (Brunner and Rechberger 2004; Allesch and Brunner 2015). We are the first ICU that applied an MFA to identify environmental hotspots in the hospital context at the department level. We have recently published the results of this MFA (Hunfeld et al. 2022). This MFA provides the necessary information for intensive care in its desired transition from a linear to a circular system, with detailed insights into materials mass, carbon footprint, agricultural land occupation and water usage related to the products that are used in the intensive care unit.
From the MFA, we identified multiple environmental hotspots. This paper will describe how the intensive care of Erasmus MC improved its sustainability by changing three environmental hotspots: gloves, gowns and CRRT bags and their packaging.
From Hotspots to Three Cases
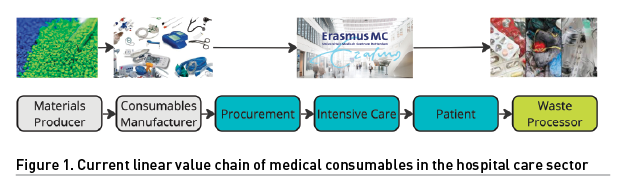
To approach the transition towards a circular hospital from a holistic view, we set up a multidisciplinary consortium comprising partners from an academic hospital (Erasmus MC), a technical university (TU Delft) and a university of social sciences (Erasmus University Rotterdam). Within the circular economy, co-creation and collaboration are key and ideally, co-creation and collaboration involve the whole value chain (Figure 1). Our consortium is built around the hospital value chain and serves an extensive network (from materials producers to waste processors). The relevance of this value chain is described previously (Hinrichs-Krapels et al. 2022) and concludes that if we want to move towards more radical and long-term shifts in designing interventions towards transitions, a quadruple-helix approach will be necessary. This will involve cross-disciplinary and cross-sectoral research and implementation across (1) industry, (2) government, (3) academia, and (4) the public. Together with master students from Industrial Design Engineering and Behavioural Economics, we examined how to improve three environmental hotspots. We will describe these cases in more depth below. The case description will follow the following items: environmental hotspot analysis, R approach (Figure 2), redesign, behavioural change (if applicable) and supply chain implications.
The final phase of a case consists of implementation of the redesigned product in the ICU. In our setting, this is guided by the green team of the ICU. This green team is vital to harnessing employee expertise, motivating, and finding new and better ways to transition (Trent et al. 2023). Our ICU green team is a diverse team, representing the ICU medical profession by nurses, doctors, and pharmacists, together with expertise from infection prevention, logistics and procurement, and project management leadership.
Gloves
Hotspot analysis
The largest number of individual units procured for the ICU are nitrile gloves, with an average of around 108 gloves being used daily per patient treated in the ICU. Their aggregated weight also makes up more than 12% of the total weight of disposable medical material used. From the impact assessment, nitrile was highlighted as the material with the highest impact intensity in terms of carbon footprint (9.3 kg CO2-eq/kg nitrile) and water usage (0.5 m3 water/kg nitrile) (Circular Intensive Care Unit Erasmus MC, Report Metabolic 2021). Given the high environmental impact of gloves, we aimed to redesign their use.
R-approach
Refuse and Reduce will result in the largest impact. This requires a change in the behaviour of the medical staff. In our ICU, it is currently common to wear gloves for all procedures. We recently started a new campaign, together with the infection prevention department, showing medical staff when gloves are needed. For example, in a non-isolation patient's room: only wear gloves when dealing with excreta (e.g., bodily waste including faeces, urine, and mucus), medication (administration of chemotherapy), and blood. To refuse and reduce the use of gloves, we combined this campaign with a newly designed glove box. Rethink is the other R-strategy related to the gloves. Both the packaging (short-term solution) and the material (nitrile, long-term solution) require a more sustainable redesign.
Redesign
This research and design project addressed the problem from three different perspectives: user-centred, product-centred, and supply-centred (vd Berg et al. 2022). The users of the gloves were observed during their work to identify the problems that occur. The product was analysed by trying to take out the gloves one by one from the cardboard dispenser. Due to poor design and packaging, the gloves are difficult to dispense one by one. By analysing the waste, it became clear that around 6% of the gloves end up in the waste unused. The project resulted in a redesign of the current glove dispenser with a focus on five aspects: 1) dispensing one glove at a time, 2) dispensing gloves at the cuff, according to infection prevention rules, 3) vertical position of the box, which is more ergonomic to the user, 4) the use of colours on the dispenser for different sizes, so nurses will see at a glance which size gloves the box contains, and 5) a small V-shaped opening which makes the undesirable behaviour of placing gloves back almost impossible. The final glove box design can provide benefits for multiple stakeholders within the healthcare system and also outside the ICU.
Supply chain implications
The case highlighted two important interfaces with the supply chain: First of all, in line with the above analysis, a redesign and manufacturing of a new type of dispenser and a better approach to how the dispensers are filled (stacked instead of bunched up). At the same time, another interface with the supply chain is to ask the market to design and manufacture (at scale) different types of gloves consisting of material with less environmental impact (e.g. a different type of nitrile [Hunfeld et al. 2022]).
Gowns
Hotspot analysis
Our MFA showed that 16 single-use gowns per ICU patient per day are used. Of all personal protective equipment, gowns were the largest contributor to CO2 emissions during the first six months of the COVID-19 pandemic (Rizan et al. 2021), which means that a reduction in gown usage is an important step towards a circular hospital.
R-approach
We aimed to Reduce gown usage in two distinctive ways: a transition from wearing gowns to wearing aprons when working with non-isolation patients and - when working with these non-isolation patients - to only wear aprons when dealing with excreta and blood. To achieve this goal, behavioural change in ICU personnel was needed.
Redesign
The case of gowns did not need a redesign. There are aprons and washable gowns available on the market.
Behavioural change
To facilitate behavioural change, we combined a policy change and informational campaign with nudging. To examine the effect of two different nudges on gown usage amongst ICU personnel, we ran a field experiment at Erasmus MC (consisting of 4 ICU Units: A, B, C and D). Specifically, we tested the effect of a visual prime and social norm nudge on apron usage. Upon the introduction of the policy change, for 1.5 weeks, we counted how many aprons were used during the day shift in non-isolation rooms across the ICU (i.e., baseline measurement). Next, we introduced a visual prompt sticker and prime (i.e., banner) in Units A and B and a social norm sticker in Units C and D. The social norm sticker stated that 81% of ICU personnel from a comparable hospital preferred to act sustainably and only wear an apron when needed. To examine the effectiveness of our interventions, for a period of 1.5 weeks, we counted how many aprons were used. To examine the effect of each nudge independently, we distinguished between Units A and B and Units C and D. We found an 8 percent point decrease in apron usage between the pre-intervention measurement and the post-intervention measurement in the visual prime condition. Unexpectedly, the social norms stickers led to a 6 percent point increase in apron usage. Neither differences were statistically significant. We will continue our search for ways to encourage more sustainable behaviour amongst ICU employees. We have conducted a series of interviews with ICU personnel to involve the employees themselves in this behavioural transition. Another step forward would be to move from Reduce to Reuse by moving from single-use aprons to washable aprons.
Supply chain implications
This case shows multiple implications for the supply chain. One implication is a switch from single-use gowns to less polluting washable gowns (Vozoola et al. 2018). For Erasmus MC, this requires a tender because of the academic hospital status. This takes time, so Erasmus MC decided to switch to aprons in the meantime. These aprons fulfil the infection prevention rules regarding non-isolation patients. However, gowns are needed for isolation patients. At the moment, we don't have information about the environmental impact of aprons compared to washable gowns. This information is needed before we can set out a future policy: switching to washable gowns for all patients or the use of washable gowns for isolation patients only?
CRRT bags and their packaging
Hotspot analysis
One of the low-hanging fruit cases are the continuous renal replacement therapy (CRRT) bags with their packaging. On average, the ICU of Erasmus MC uses 30,000 5-litre bags (Fresenius Medical, 's-Hertogenbosch, the Netherlands) per year. This adds up to 3,600 kg of plastic waste. Since this is a clean waste stream that can be separated easily from other waste streams, we asked the waste processor if it was possible to create a separate logistics recycle stream for the CRRT packaging and the bags. The waste processor analysed the type of plastic, and both the bag and the packaging appeared to be a pure polypropylene polymer suitable for high-quality recycling. The connectors at the bottom of the bag have to be removed because they consist of a different type of plastic, unsuitable for this type of recycling.
R-approach
For this hotspot, the Recycling of empty CRRT bags (without connectors) and their packaging is a fitting strategy.
Redesign
In this case, there was no need to redesign the product itself. However, a special cutting tool was designed to split the connectors from the bag. Also, a box was made to store empty bags and packaging. This box is attached to the CRRT trolley that is parked outside the patient's room containing new CRRT bags. The ICU nurses are asked to put the CRRT bag packaging in this box as well as the empty bags after having removed the connectors.
Supply chain implications
This case also highlighted two interfaces with the supply chain. First of all, a reverse, closed-loop supply chain needs to be developed to recycle the packaging. Second, collaboration with the supplier needs to be initiated to redesign the CRRT bag in such a way that the connectors can be easily cut off/torn off to enable recycling of the CRRT bag itself. It also stresses the importance of the use of pure plastics that can be recycled for both packaging and the product itself. This should be taken into account during tenders.
Summary: Lessons for the Future
Our three cases show that the transition towards circular intensive care requires a total value chain approach. Collaboration and co-creation with academic partners and industrial partners (manufacturers, suppliers, waste processors) and users (e.g. medical staff) is essential in the change towards more sustainable products, protocols and processes. From our experience, a case usually starts within our multidisciplinary green team (Bein and McGain 2023). After the green team has defined a new case, we collect data about how many products are used on an annual basis and we ask infection prevention specialists (part of our green team) for advice regarding the case and the planned intervention. With this information, a case is then redesigned within our consortium and tested in the ICU. The final step involves the implementation of the newly designed case. This step requires a sharp focus on behaviour and communication within the ICU. Again, it is the green team that advises on the implementation and communication. With this strategy, we were able to implement many sustainable cases already. The involvement of procurement is key and in case of public procurement, alignment with the tendering calendar is an important factor to take into account. Finally, make sure that you can show data on the environmental and financial impact of a case. This helps medical staff change their behaviour.
Acknowledgements
We acknowledge Julia Pongratz, Lisanne van de Berg, Meyke Maanicus, Theo Post, and Tamarah Verhoog carrying out their master's project involving the cases described in this paper. We thank Focco Ottens (waste processor PreZero, Arnhem, the Netherlands) for the analysis of the CRRT bags.
Conflict of interest
None.
References:
Allesch A, Brunner P (2015) Material flow analysis as a decision support tool for waste management: a literature review. J Ind Ecol. 19:753-764.
Bein T, McGain F (2023) Climate responsibilities in intensive care medicine—let’s go green! An introduction to a new series in Intensive Care Medicine. Intensive Care Med. 49:62-64.
Brunner P, Rechberger H (2004) Practical handbook of material flow analysis. Lewis Publishers, Washington DC.
Circular Intensive Care Unit Erasmus MC. Report Metabolic (2021). Available on request.
Ellen MacArthur Foundation (2020) What is a Circular Economy? A Framework for an Economy that is Restorative and Regenerative. Available at https://ellenmacarthurfoundation.org/topics/circular-economy-introduction/overview.
Hinrichs-Krapels S, Diehl JC, Hunfeld N, van Raaij E (2022) Towards sustainability for medical devices and consumables: the radical and incremental challenges in the technology ecosystem. J Health Serv Res Policy. 27:253-254.
Hunfeld N, Diehl JC, Timmermann M et al. (2022) Circular material flow in the intensive care unit - Environmental effects and identification of hotspots. Intensive Care Medicine.
Karliner J,
Slotterback S, Boyd R et al. (2022) Health care’s climate footprint: the health
sector contribution and opportunities for action. Eur J Public Health. 30(Suppl_5):ckaa165-843.
Kirchherr J, Reike D, Hekkert M (2017) Conceptualizing the circular economy: an analysis of 114 definitions. Resour Conserv Recycl. 127:221-232.
McGain F, Muret J, Lawson C, Sherman JD (2020) Environmental sustainability in anaesthesia and critical care. Br J Anaesth. 125:680-692.
McGain F, Burnham JP, Lau R et al. (2018) The carbon footprint of treating patients with septic shock in the intensive care unit. Crit Care Resusc. 20:304-312
Reike D, Vermeulen W, Witjes S (2018) The circular economy: new or refurbished as CE 3.0? Exploring controversies in the conceptualization of the circular economy through a focus on history and resource value retention options. Resour Conserv Recycl .135:246-264.
Rizan C, Reed M, Bhutta MF (2021) Environmental impact of personal protective equipment distributed for use by health and social care services in England in the first six months of the COVID-19 pandemic. Journal of the Royal Society of Medicine. 114(5):250-263.
Steenmeijer MA, Rodrigues JFD, Zijp MC, Loop SLW der (2022) The environmental impact of the Dutch healthcare sector beyond climate change: An input–output analysis. The Lancet Planetary Health. 6(12):e949-e957.
Transition to a sustainable healthcare sector (2019) Gupta Strategists. Available at https://gupta-strategists.nl/en/research/een-stuur-voor-de-transitie-naar-duurzame-gezondheidszorg
Trent L, Law J, Grimaldi D (2023) Create intensive care green teams, there is no time to waste. Intensive Care Med.
vd Berg L et al. (2022) Towards greener ICUs: Redesigning the use of disposable gloves. Abstract. Available at https://www.heps2022.com/_files/ugd/3d0da7_49a6b09a01744a3380aab7a0b79cdf88.pdf
Vozzola E, Overcash M, Griffing E (2018) Environmental considerations in the selection of isolation gowns: a life cycle assessment of reusable and disposable alternatives. American journal of infection control. 46(8):881-886.
World Health Organization (2018) Healthcare waste. Available at https://www.who.int/news-room/fact-sheets/detail/health-care-waste


















