




ICU Management & Practice, Volume 21 - Issue 4, 2021
 PRINT OPTIMISED
PRINT OPTIMISED
Introduction
Most diseases and syndromes are differently expressed in men and women. While women represent nearly 80% of cases of autoimmune disease, men are the most affected by cancer (Ortana et al. 2016; Cook et al. 2009). This sex dimorphism affects patients admitted to the intensive care unit (ICU). Indeed, males represent 60% of ICU patients (Samuelsson et al. 2015). The mechanisms underlying this unequal distribution are based on both sex as a biological entity determined by chromosomal, hormonal, and immunological differences, and gender as a social construct, resulting in disparities in co-morbidities and access to healthcare.
The incidence and severity of a given disease may vary according to the sex of patients, as recently observed during the Coronavirus-19 (COVID-19) pandemic, with men developing more severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia than women (Lakbar et al. 2020). The acknowledgment of sex dimorphism could therefore be considered as the first step in personalised management of ICU patients (Lakbar and Leone 2021). Here, we briefly overview the current literature on the topic to discuss sex differences in patients admitted to the ICU.
Definition
In 1955, the controversial sexologist John Money was the first to use the term “gender” to describe human characteristics and behaviours. This term opened a new field of scientific research. In the recent literature, sex refers to the set of morphological differences between males and females, including primary and secondary sexual characteristics, anatomical, biological and genetic specificities.
Epidemiology
Infectious diseases and sepsis
Sex dimorphism is reported in infectious diseases (Gay et al. 2021), which are among the most common diseases encountered in ICUs. Men are predominantly affected by both sepsis and septic shock.
A 24-hour point prevalence study collecting global data revealed that out of 15,202 patients, 54% had a suspected or known infection (Vincent et al. 2020). Men were more likely to develop infection than women with a mean annual relative risk (RR) of 1.28 (confidence interval 95%, (CI95) [1.24-1.32]) (Martin et al. 2003). Sex differences are reported for the release of inflammation mediators. In response to lipopolysaccharides (LPS), peripheral blood mononuclear cells from men produce more tumour necrosis factor (TNF) (Asai et al. 2001), and in patients with sepsis, men have higher serum TNF concentrations and lower interleukin (IL)-10 concentrations than women (Schröder et al. 1998). This hyper-responsiveness of male-derived cells to LPS was suggested as a potential mechanism whereby men are more susceptible to sepsis than women. In an experimental model of Coxiella burnetii infection, our group showed that only 14% of the modulated genes were sex-independent, and the remaining 86% were differentially expressed in males and females, underlying the interplay between sex and host response to infection (Textoris et al. 2010).
Over the last decade, large-scale studies reported a higher incidence of sepsis in men than women. The agents responsible for sepsis differ in men and women. Bacteraemia due to Staphylococcus aureus and Pseudomonas aeruginosa are more frequent in men than in women (Benfield et al. 2007; Al-Hasan et al. 2008). Conversely, 60% of Escherichia coli bacteraemia occur in women (Laupland et al. 2008).
In sepsis, the source of infection differs in men and women. Respiratory tract is identified as source of infection in 36% of cases in men and 29% of cases in women (p<0.01), whereas the infection of genitourinary tract is predominant in women (35% vs. 27% for men, p<0.01) (Laupland et al. 2008). Anatomical differences partly explain these findings.
Non-infectious diseases and syndromes
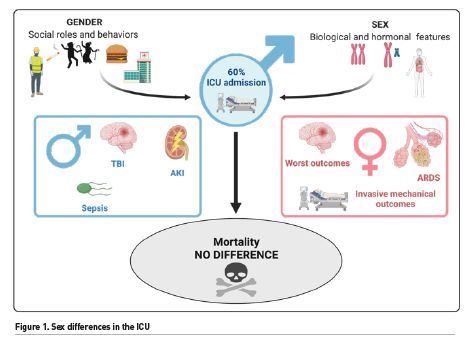
Traumatic brain injury (TBI) is a public health concern. Epidemiological studies show that men have an increased relative risk to suffer a TBI compared with women in the general adult population of the United States until 75 years-old (Faul and Coronado 2015). Acute kidney injury (AKI) has a variable prevalence in ICU. In observational studies, sex affects directly the risk to develop AKI in the ICU patients. The risk was significantly higher in men than in women (OR 1.23; 95% CI [1.11-1.36]) (Neugarten and Golestaneh 2018). Among 25,998 patients (58% of men), the use of renal replacement therapy was significantly higher in men than in women (OR, 1.28; 95% CI [1.16-1.42] (Valentin et al. 2003). All in all, the female hormonal status probably protects against AKI. In a French nationwide cohort study, men represented 67.7% of patients developing acute respiratory distress syndrome (Papazian et al. 2021).
Surprisingly, while the incidence of these diseases or syndromes is sex-dependent, there was, in most conditions, no difference in mortality between both sexes. The FROG-ICU study was performed on 2,087 patients, including 726 women and 1261 men, in 19 hospitals in France and Belgium (Hollinger et al. 2019). A similar one-year mortality after ICU admission was found between men and women (34.9% vs. 37.9%, p=0.18). Same results were found regarding ICU mortality and 28-day mortality. This finding is not confirmed in specific syndromes like ARDS, an increased 90-day mortality of males being reported (OR 1.104 95% CI [1.014-1.200]) (Papazian et al. 2021). Besides biological data that explain the sex dimorphism in the incidence of critical illness according to sex, social behaviours are a cornerstone of these differences (Figure 1).
Gender Behaviours
Differences in social behaviours, expressed as gender effect, may interfere with sex to highlight differences between men and women facing critical illness. As an example, differences in the prevalence of smoking between men and women could explain the increased risk of tobacco-associated respiratory diseases and infections in men than in women (Garrett et al. 2011).
Lifestyle is influenced by gender. In a population of 761 adolescents, young girls presented lower performance in physical exercise and physical and psychological wellbeing but higher vegetable consumption and greater satisfaction in educational context (Boraita et al. 2020). Such stereotypes could influence behaviours and affect susceptibility to infection.
Regarding access to healthcare, gender inequalities are persisting. The prevalence of perceived unmet healthcare is higher in women than in men. In 2019, the #LancetWomen movement was created to promote gender equality worldwide and highlight the inequality in science, medicine, and global health between men and women (Shannon et al. 2019). For patients with respiratory failure, a study showed that men had a higher probability of receiving mechanical ventilation (Schultz and Karagiannidis 2019). Inequity in the setting of ventilator parameters was also observed: being a woman is even a risk factor to receive an inappropriate and unsafe ventilation setting (Swart et al. 2021). Authors highlighted the need for a campaign “Save the life of Females in ICU”.
Another concern is related to the design of randomised controlled trials. For safety concerns, they often exclude women of childbearing age. Hence, most drugs are essentially tested in men and are given to both men and women. In septic patients with tachycardia, a recent meta-analysis showed that beta-blocker use was associated with favourable outcomes (Hasegawa et al. 2021). However, in experimental murine models of sepsis, our group showed a sex-dimorphism of beta-receptors, suggesting that beta-blockers may be beneficial in septic males and deleterious in septic women (Mathieu et al. 2018; Tran et al. 2019). Thus, there is a need to refine our research criteria to test the drugs both in men and women.
Conclusion
Sex seems to be a major determinant in the trajectory of patients developing critical illness. Both biological and social factors play a role in this trajectory. Generally, male sex seems to be associated with an increased risk to develop severe forms of diseases mainly due to an inappropriate immune response. However, both the number and effects of interventions are unequally distributed between men and women, interplaying with outcomes. Considering sex as a critical variable should be recognised as one of the first steps of personalised medicine in the ICU.
Conflict of Interest
ML served as lecturer for MSD, Aspen and consultant for Amomed, Gilead. AL an IL do not have any conflict of interest.
References:
Al-Hasan MN, Wilson JW, Lahr BD et al. (2008) Incidence of Pseudomonas aeruginosa bacteremia: A population-based study. Am J Med, 121(8):702‑708.
Asai K, Hiki N, Mimura Y et al. (2001) Gender differences in cytokine secretion by human peripheral blood mononuclear cells: Role of estrogen in modulating LPS-induced cytokine secretion in an ex vivo septic model. Shock, 16(5):340‑343.
Benfield T, Espersen F, Frimodt‐Møller N et al (2007) Increasing incidence but decreasing in-hospital mortality of adult Staphylococcus aureus bacteraemia between 1981 and 2000. Clin Microbiol Infec, 113(3):257‑263.
Boraita RJ, Ibort EG, Torres JMD et al. (2020) Gender differences relating to lifestyle habits and health-related quality of life of adolescents. Child Ind Res, 13(6):1937‑1951.
Cook MB, Dawsey SM, Freedman ND et al (2009) Sex disparities in cancer incidence by period and age. Cancer Epidemiol Biomarkers Prev, 18(4):1174‑1182.
Faul M, Coronado V (2015) Epidemiology of traumatic brain injury. Handb Clin Neurol, 127:3‑13.
Garrett BE, Dube SR, Trosclair A et al (2011) Cigarette smoking - United States, 1965-2008. MMWR Suppl, 60(1):109‑113.
Gay L, Melenotte C, Lakbar I et al (2021) Sexual dimorphism and gender in infectious diseases. Front Immunol, 12:698121.
Hasegawa D, Sato R, Prasitlumkum N et al (2021) Effect of ultrashort-acting β-blockers on mortality in patients with sepsis with persistent tachycardia despite initial resuscitation: a systematic review and meta-analysis of randomized controlled trials. Chest, 2159(6):2289-2300.
Hollinger A, Gayat E, Féliot E et al (2019) Gender and survival of critically ill patients: results from the FROG-ICU study. Ann Intensive Care, 9(1):43.
Lakbar I, Luque-Paz D, Mege JL et al. (2020) COVID-19 gender susceptibility and outcomes: A systematic review. PLoS ONE, 15(11):e0241827.
Lakbar I, Leone M (2021) An insight depicting estradiol pathway in sepsis. Minerva Anestesiol, 87(5):505-507.
Laupland KB, Gregson DB, Church DL et al. (2008) Incidence, risk factors and outcomes of Escherichia coli bloodstream infections in a large Canadian region. Clin Microbiol Infect, 14(11):1041‑1047.
Martin GS, Mannino DM, Eaton S et al. (2003) The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med, 1348(16):1546‑1554.
Mathieu C, Desrois M, Kober F al (2018) Sex-mediated response to the beta-blocker landiolol in sepsis: an experimental, randomized study. Crit Care Med, 46(7):e684‑e691.
Neugarten J, Golestaneh L (2018) Female sex reduces the risk of hospital-associated acute kidney injury: a meta-analysis. BMC Nephrology, 819(1):314.
Ortona E, Pierdominici M, Maselli A et al (2016) Sex-based differences in autoimmune diseases. Ann Ist Super Sanita, 52(2):205‑212.
Papazian L, Pauly V, Hamouda I et al (2021) National incidence rate and related mortality for acute respiratory distress syndrome in France. Anaesth Crit Care Pain Med, 40(1):100795.
Samuelsson C, Sjöberg F, Karlström G et al. (2015) Gender differences in outcome and use of resources do exist in Swedish intensive care, but to no advantage for women of premenopausal age. Crit Care, 19:129.
Schröder J, Kahlke V, Staubach K-H et al. F (1998) Gender differences in human sepsis. Arch Surg, 1133(11):1200‑1205.
Schultz MJ, Karagiannidis C (2019) Is gender inequity in ventilator management a "women's issue"? Eur Respir J, 254(4):1901588.
Shannon G, Jansen M, Williams K et al (2019) Gender equality in science, medicine, and global health: where are we at and why does it matter? Lancet, 393(10171):560‑569.
Swart P, Deliberato RO, Johnson AEW (2021) Impact of sex on use of low tidal volume ventilation in invasively ventilated ICU patients-A mediation analysis using two observational cohorts. PLoS One, 16(7):e0253933.
Textoris J, Ban LH, Capo C et al. (2010) Sex-related differences in gene expression following Coxiella burnetii infection in mice: potential role of circadian rhythm. PLoS ONE, 5(8):e12190.
Tran TT, Mathieu C, Torres M et al (2019) Effect of landiolol on sex-related transcriptomic changes in the myocardium during sepsis. Intensive Care Med Exp, 17(1):50.
Valentin A, Jordan B, Lang T et al. (2003) Gender-related differences in intensive care: a multiple-center cohort study of therapeutic interventions and outcome in critically ill patients. Crit Care Med, 31(7):1901‑1907.
Vincent JL, Sakr Y, Singer M et al (2020) Prevalence and outcomes of infection among patients in intensive care units in 2017. JAMA, 2323(15):1478.















