



HealthManagement, Volume 19 - Issue 3, 2019
 PRINT OPTIMISED
PRINT OPTIMISED
A leadership model for the health care sector
In medical institutions, leaders are required to ensure, through delegation of responsibility, that working conditions are characterised by interdisciplinary thinking, team-oriented work and ongoing improvement.
Leaders in the health sector must be aware of
the fact that hospitals operate in a market,
which is not in fact a market in the classic
competitive economic sense. Nevertheless, in a
medical world characterised by increasing patient
expectations, expensive innovative treatment opportunities
and limited budgets hospital managers
are forced to perform higher medical quality and
containing costs simultaneously.
You might also like: Trust-abundant team principles
In this complex VUCA world (volatile, uncertain,
complex, ambiguous), convincing and successful
leadership conveys binding values and norms (why
do we do something?) and creates legitimation (for
whom do we create what value-added?), provides
orientation (what are we doing?) and how to transform
plans into successful organisational development
(how do we do it?).
Those in leadership positions can obtain assistance
through the leadership and organisational
approach of the CKM leadership model for valueoriented
management. It serves as an orientation
for action and a compass for managing medical
organisations.
Initial situation
Internationalisation, digitalisation, changing societal
values, the impact of the economy on medicine,
and demands for ecological sustainability are all
confronting “leadership” with new challenges. What
constitutes “good” leadership? When can leadership
be regarded as “successful” and what characterises
a good leader? Can one learn to lead, what
leadership instruments have stood the test of time
and what behavioural rules provide support along
the path to successful leadership? Leadership is
also always a reflection of the political, societal
and economic framework and prevailing situation.
It is also influenced by the specifics of a particular
industry, which applies all the more to the health
care sector (see Figure 1).

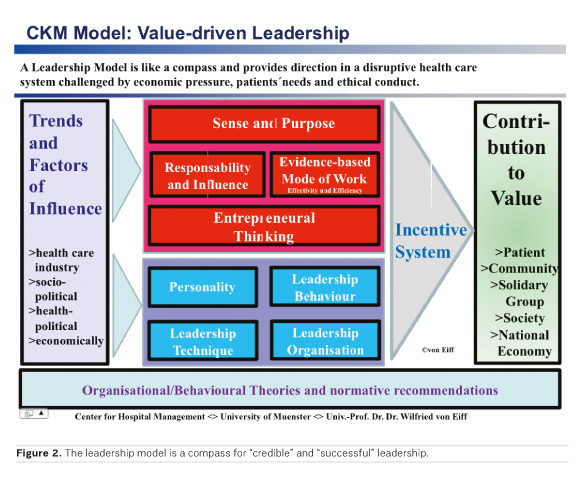
Below, the CKM Leadership Model is described in
terms of its basic dimensions and design elements
(see Figure 2).
External conditions, that is, political, economic
and societal trends, as well as the dynamics of the
health sector, substantially determine the nature and
organisation of leadership in medical institutions.
You might also like: Leading change and value
In this context, the management of hospitals,
rehabilitation clinics and nursing homes find
themselves in a difficult balance between financial
constraints, a shortage of qualified personnel,
digitalisation, employee expectations and calls
for family-friendly working conditions. In addition,
there are rising quality requirements and a growing
demand for medical services by multimorbid, chronically
ill and aged people. As a reaction to such developments,
there are changes in the content and
nature of work, qualification profiles, work processes
and forms of cooperative work. Furthermore, altogether
new forms of jobs are also emerging.
Values and behavioural guidelines for leadership
are represented through the formational dimensions
of sense and purpose, responsibility, entrepreneurial
thinking and resource orientation (= efficiency and
effectiveness; evidence-based practice).
The following questions are to be answered:
“What mode of thinking characterises leadership?”
and “What ethical rules guide leadership?”
and “How can the efficiency and effectiveness of
clinical processes be ensured in order to achieve
sustainable financing for a medical business?” and
“What are the key performance indicators for measuring
and evidence-based steering of all medical
and nursing activities?”
Sense and purpose determine the legitimation of
an enterprise in a competitive market and within the
community. The sense and purpose demonstrate
what the client (patient, relatives, referring doctor,
cooperation and business partner, community) can
justifiably expect from an enterprise. And this is an
internally fundamental source of intrinsic motivation
for employees. In dilemma situations of decisionmaking
where managers are forced to decide, for
instance between financial limitations and patient
needs, “sense and purpose” assumes the role of
“referee institution,” in terms of a “meta level goal:”
In case of doubt, patient comes first!
In an exceptional situation, customers (patients
and relatives) experience such “moments of truth”
and sense the social quality of a corporate culture.
You might also like:Compassion
The CKM leadership model advises “sense
and purpose” to focus not primarily on economic
constraints, but on patient and family-centredness,
as well as on patient experience (see Figure 3).
Responsibility on the part of leaders in the
medical business are primarily concerned with the
wellbeing of the patient. Their decisions and actions
are subject to the medical ethics principle: primum
nihil nocere (first do no harm), patient wellbeing,
autonomy and dignity. They use economic principles
(eg causality principle, equal-treatment principle) in
order to overcome the challenges presented by the
health system with regard to sustainable finance,
as well as an equitable allocation of health services.
The patient is not an autonomous, decision-making
client, but a sick person with anxiety and
pain, often in a physical and psychological borderline
situation. Accordingly, the service process is particularly
subject to ethical and behavioural guidelines.
The leadership principle of shareholder value is the
short-term orientation as a managerial philosophy,
and revenue maximisation and thinking in terms
of quarterly results is entirely inappropriate for the
medical industry. By contrast, the stakeholder-value
approach, with particular attention being paid to
patient risks and fairness within a solidarity-oriented
financial system, is the philosophy of choice.
Responsibility is the central controlling instrument
of an entrepreneurial incentive system: the assumption
of responsibility is both expected and rewarded
(financially and ideally), and structures associated
with an organised lack of responsibility will not be
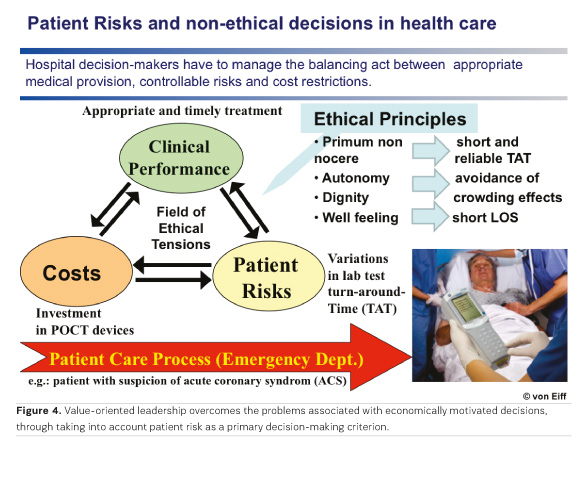
tolerated. Value-oriented leadership in the medical
business is committed to medical-ethics principles.
As a criterion of ethical evaluation for each managerial
decision, what matters is the extent of risk that
the patient bears, if, for example, there is rationing
of medical services needed for appropriate treatment
for cost reasons (see Figure 4). The more
emphasis hospital manager’s place on cost containment,
budget restrictions and economic criteria, the
more medical quality will decrease and, simultaneously,
the risk of the patient suffering harm rises.
Entrepreneurial thinking and behaviour aims at
securing innovation and the ability of the organisation
and of the community to survive. An organisational
culture, in which entrepreneurial thinking has
a compelling value, is characterised by a constructive
handling of errors, and oriented towards problem
solving and contributing to continuous improvement.
Entrepreneurial leadership is constructively
aligned with the “New Management Paradigm”,
according to which rising quality in the medical
industry, together with a tendency towards declining
cost, is to be achieved. Entrepreneurial leadership
is also constructively aligned with “New Management-Entrepreneurial
Awareness and Behaviour” and
is necessary at all levels of an organisation and has
to apply across professional groups and boundaries.
This is conditional on the assumption of responsibility
by colleagues as well (“Every Employee a
Manager“).
The process is ensured through the participation
of colleagues who are capable of delegation
in decision-making processes, through setting up
task areas, which are suitable for delegation, with
clearly defined decision-making autonomy, as well
as through clinically oriented compliance management.
Entrepreneurial leadership also aims at
including and integrating employees in decision-making
processes, in order to solve problems and
contribute to continuous improvement.
Resource-orientation commits the institutions
within the health system to ensuring efficiency
and effectiveness, because, in the health sector,
wastage, redundant (double) work and errors lead to
investment and quality gaps, which jeopardise the
sustainability of financing. In the health sector, the
generally accepted principle for a market economy
of “creative destruction” leads to patient risks and
is associated with additional costs, which ultimately
cause the care situation to deteriorate in the future.
Effective leadership converts “sense and aim” into
goal-oriented behaviour, overcoming complexity
through coordination and resolving goal conflicts
constructively.
The dimension of leadership competence
comprises the formational attributes of leadership
techniques, leader behaviour & personality and
leadership organisation. The central questions are:
“What attributes characterise leadership and how
can they be influenced and formed? What leadership
instruments have proven their worth over time?
What relationship prevails between successful leadership
and personality?”
Leadership techniques
Leadership techniques subsume leadership
methods and instruments into goal-oriented, transparent
and understandable control of colleagues
and employees. One method is that of using structured
processes to recognise a problem and solve
it in a systematically understandable and transparent
manner. An appropriate methodology, as a
systematic approach supporting decision-makers in
managing the process from identifying a problem-to-problem
solving, ensures that a leader can understand
at any stage of the decision-making process,
how an intermediate result arises. By so doing,
learning processes for future decision-making, in
the sense of experience formation, are possible.
Suitable instruments include surveys, analysis,
communication and decision-making techniques,
which can all provide tangible support in achieving
leadership objectives.
The leadership technique of “Management by
Objectives“ (MbO) entails a recommendation for a
structured process of objective formation, agreement
and control, and further employee development
on the basis of constructive criticism. As leadership
instruments, the documented agreement on
objectives, evaluation systems, reward systems and
personal development systems, are used.
The MbO concept works on the basis that agreed upon
objectives, in combination with a reward and
personal-development system that is regarded as
fair, foster the intrinsic motivation of employees.
The basic condition for the successful implementation
of MbO is firstly the establishment of organisational
units that are capable of delegation, and
which create congruence between task (objective),
competence and responsibility. Secondly, a transparent
system comprises agreement on objectives,
and is accompanied by performance control and
employee development.
The CKM leadership model provides leaders in
the institutions of medical service providers with
the normative, strategic behavioural recommendation
not to form any goal-agreements with an exclusively
economic focus, because this would generally
lead to ethical conflicts. Thus, agreements on
the quantity of certain types of operation (eg total
hip replacement) run contrary to the requirements
of indications quality, and transgress the ethical
maxim of “primum nihil nocere.”
Leadership behaviour
Leadership behaviour characterises the active
communicative impact of a leader on employees
in terms of goal attainment. This also entails the
balancing act of harmonising an employee orientation
(degree of fulfilment of employee expectations)
and a task orientation (importance of the enterprise’s
requirements of its employees). Successful
leadership behaviour is based on proven rules of
communication, eg establishing rituals, providing
feedback and ensuring transparency pertaining
institutional needs, as well as employee expectations
(career opportunities, family-friendly workplace
conditions, work life balance).
Personality and leadership
All individuals have their own unique personality
profile. Even in antiquity, philosophers such as
Hippocrates and Empedocles attempted to create
a typology of human behaviour, in order to predict
how certain personality types could be expected
to behave. The early typologies so derived entailed
four basic types: choleric, sanguine, melancholic
and phlegmatic.
The personality type determined the work,
communication and behavioural style. This style is
situational and influenced particularly by work stress,
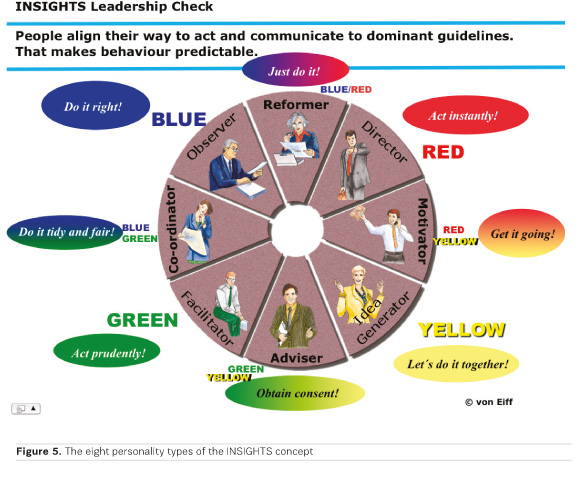
time pressure, errors and so on. As an instrument
for analysing and predicting the work, communication
and behavioural style of a particular person, the
INSIGHTS Leadership Check has proven its worth.
INSIGHTS refer to the interrelationship between
personality and successful leadership on the basis
of eight standardised personality types (see Figure
5), whose typical modes of behaviour in typical situations
can be categorised into normal situations,
stressful situations and those with extreme stress.
In the context of the dimension of an incentive contribution
system, the following question is posed:
“what function and significance does the corporate
culture have and how is it possible to develop
a goal-oriented incentive system that is regarded
as fair by all participants?”
The incentive system comprises monetary
components (salary, special payments, bonuses,
overtime), contains fringe benefits (child care,
employer-sponsored housing benefits, public transport
tickets), includes the working conditions (work place design and equipment, working times, holiday
regulations) and also regulations for personal development
(continuing education, career opportunities
as specialists or in management) as well as a
system for internal company suggestions.
The corporate culture is characterised by the
manner in which the following are dealt with:
conflicting opinions, suggestions for improvement,
employee initiatives, errors, resource wastage and a
failure to disclose information. Formulated behavioural
principles and leadership guidelines render an
enterprise’s culture transparent and understandable.
What is important is that any contravention
of the corporate culture values be followed up and
investigated. The incentive-contribution system and
corporate culture are the sources of motivation and
willingness to perform.
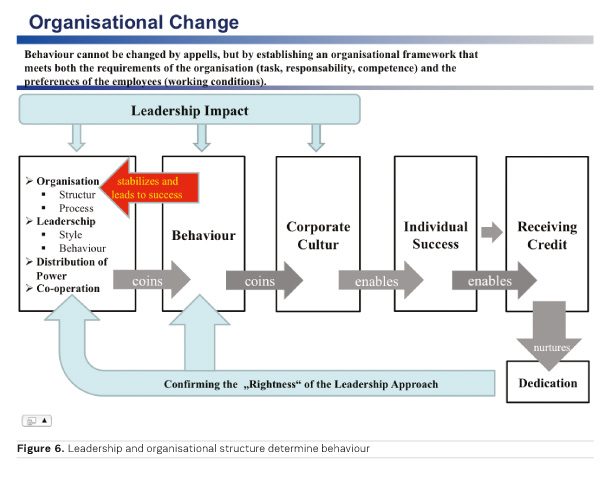
The CKM model is based on the “StructureBehaviour
Theory of Motivation” (von Eiff 2018).
According to this theory, behaviour is not changed
through appeals alone, but rather through the
formulation of conditions (organisational structure,
work conditions, rules of corporate culture,
forms of cooperative work, power relationships), all
of which enable employees to develop enthusiasm
for their work.
Leadership has the primary function of avoiding
demotivation (lack of feedback, no evident purpose
of the work, the expertise of employees is not
utilised, obviously dysfunctional work processes
are not improved). Through partial autonomy, the
formation of work and decision-making processes of
employees can be experienced successfully within
defined competence fields through their own decisions,
which fosters recognition and commitment
(see Figure 6).
The dimension of valued added through leadership
(with regard to the patient, community, solidarity
system, economy) considers the following
question: “What value is added by leaders in terms
of reasonable stakeholder expectations?” Accordingly,
leaders not only have a responsibility for
employees and enterprises, but must also take
account of the impact of their decisions on society
and the community.
A hospital is part of the infrastructure of a region
and contributes to the security and quality of life of
the citizens. As an employer, its duty is to provide
attractive, stimulating and secure jobs, and such
enterprises constitute an important economic factor
within a region. With regard to health policy, the
value added by leadership is concretised though the
Triple Aim Strategy (> quality-oriented remuneration;
> population-oriented care; > patient experience/patient
care in a recovery-promoting environment)
(von Eiff 2018).
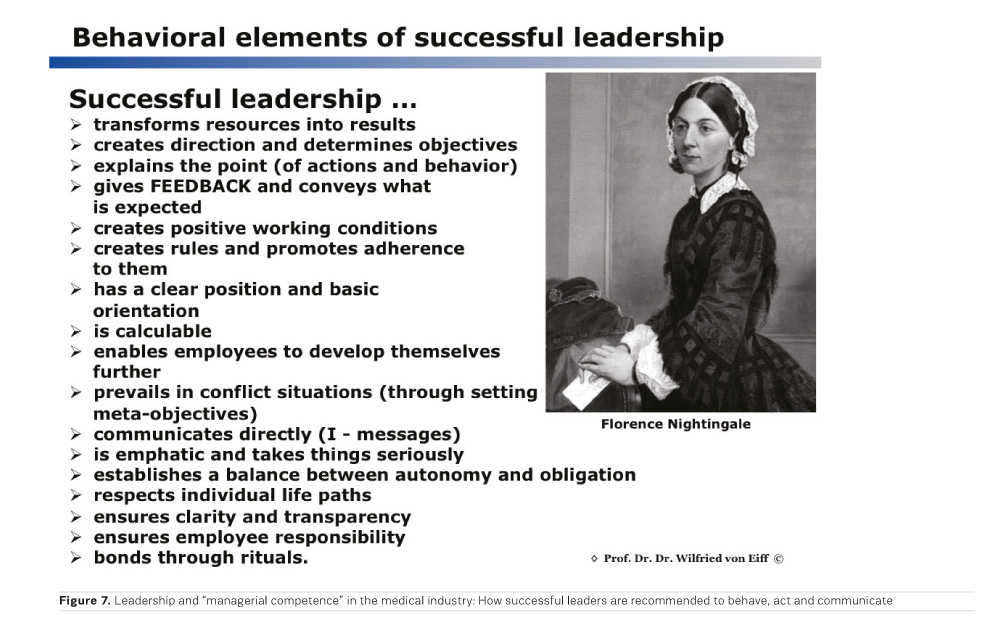
From the five dimensions of the leadership model,
specific recommendations for action can be derived,
which provide the basis for internal organisational
discussion between current and potential leaders.
Through such recommendations on leadership techniques
and behaviour (see Figure 7), leaders obtain
assistance in dealing with classic leadership situations.
That is: How do leaders communicate in a
manner that is clear and unambivalent? What typical
leadership errors should one avoid? What organisational
conditions support goal-oriented leadership?
What is the significance of rituals for determining
a stable corporate culture and how should they be
formed and formulated?
Key Points
- Leadership is a reflection of the political, societal and economic framework and prevailing situation
- In the health sector, managers must provide a high level of medical, economic and ethical competence to deal with the balance between a limited budget and a demand for suitably qualified medical services
- Before every decision, the leader must ask the question: Does my decision conform to the ethical guideline “Above all, do no harm!” or “To what risk could my decision expose the patient?”
- The CKM Leadership Model is a compass, with the help of which requirements can be targeted, structured and implemented in a sector-specific manner.
Conflicts of Interest
None
References:
von Eiff W (2018) Literature by the author













